Débit urinaire vs. créatinine :
pourquoi le facteur temps
est crucial dans la détection de la LRA
Méta-description :
La créatinine sérique est un marqueur tardif de l’atteinte rénale. Découvrez pourquoi le débit urinaire reste la mesure la plus réactive et exploitable pour la détection précoce de la LRA — en particulier en soins critiques.
Introduction
Lorsqu’il s’agit de la lésion rénale aiguë (LRA), le temps est un facteur déterminant. Plus tôt elle est détectée, plus les chances de la contrôler ou d’en inverser les effets sont grandes. Pourtant, la plupart des cliniciens s’appuient encore sur la créatinine sérique, un marqueur qui n’augmente souvent qu’une fois les lésions déjà avancées. Le débit urinaire raconte une autre histoire — et la raconte souvent en premier.
Les limites de la créatinine sérique
La créatinine sérique est facile à mesurer, mais lente à réagir. Elle peut rester dans la plage normale pendant des heures — voire des jours — après le début d’une LRA. Elle est également influencée par :
• La masse musculaire
• L’âge et le sexe
• Le niveau d’hydratation
• Certains médicaments
À l’inverse, le débit urinaire réagit en quelques heures, reflétant en temps réel la perfusion rénale et la filtration glomérulaire.
Les critères KDIGO et pourquoi le débit urinaire est essentiel
Selon les directives KDIGO sur la LRA :
• Un débit urinaire < 0,5 mL/kg/h pendant plus de 6 heures constitue un critère diagnostique de LRA — même si la créatinine est encore normale.
• De nombreuses USI passent à côté de ce signal en raison de mesures retardées, estimées ou moyennées.

Exypnos : rendre les données de débit continues et fiables
Exypnos automatise ce paramètre critique grâce à :
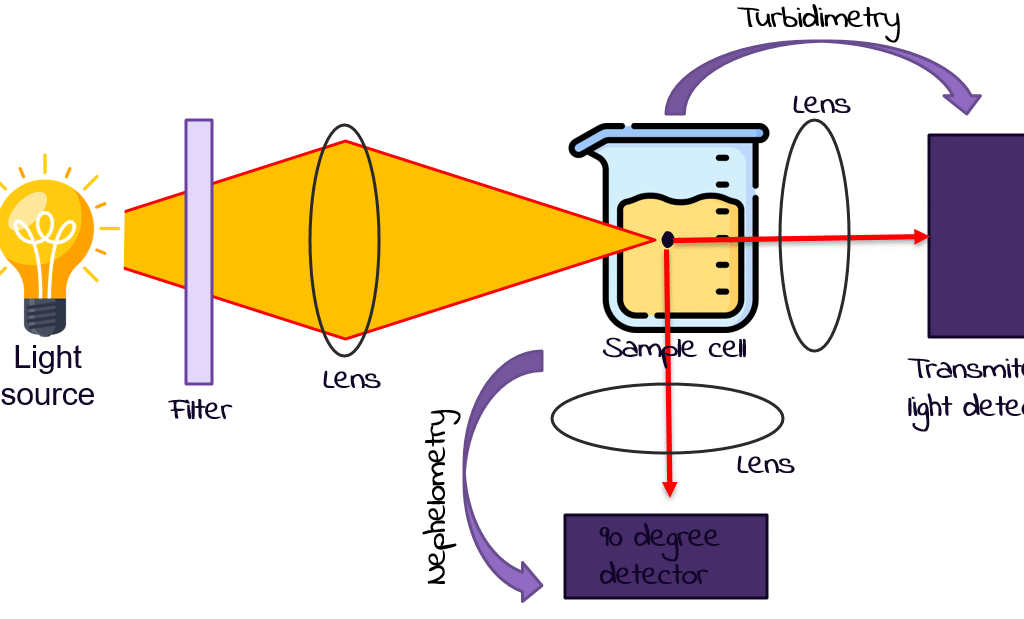
• Des capteurs optiques de débit urinaire
• Un affichage en temps réel au chevet et au poste infirmier
• Des tendances historiques et des alertes précoces pour la polyurie et l’oligurie
• Une intégration avec d’autres systèmes de score clinique
Cela permet de détecter la LRA avant que des dommages irréversibles ne surviennent — et avant qu’un pic de créatinine ne confirme trop tard ce qui avait déjà été manqué.
Conclusion clinique
Pour une intervention précoce dans la LRA, le débit urinaire doit être le premier signe vital pris en compte — et non une réflexion secondaire. En soins critiques, où le retard équivaut à une détérioration, les données en temps réel sauvent des vies.